The Carer QALY Trap
The term “Carer QALY” was coined in a paper by Mott et al. (2023) and is identified as the case where
“it is possible for an effective treatment that provides survival gains (with relatively little or no QOL gain) to appear less effective than the comparators when carer QOL is considered.”
While the term “Carer QALY trap” is new, this issue has long been known. In fact, the patient QALY trap–that extending the life of a person with a chronic disease is less valuable than extending the life of a person without one–was identified by Ubel et al. (2000) among others. The
TIlford and Tarlan (2023)editorial–citing citing Lundin and Ramsberg (2008)–uses a parable to explain the carer QALY trap as follows:
Lundin and Ramsberg portray two people on an island needing to decide whether to create a snake bite antidote that would save the life of the person after being bitten. The island snakes resided in an area with better food, and picking fruit there would increase the QoL of the two inhabitants on the island but incur the risk of being bitten while picking fruit. If one person is bitten and survives using the antidote, in the parable by Lundin and Ramsberg, the survivor would live with a very low QoL. The healthy person would then incur survivor consumption costs by having to provide for the person who survived the snake bite. The link to the carer QALY trap is straightforward; in providing for the person with the snake bite, the healthy person loses QALYs.
A similar example would be considering a treatment that would prolong the survival of a child with severe brain damage. Because QoL would be low, life extension would create few QALYs for the patient; moreover, the caregiver QoL would decline. Thus–similar to the snakebite case–there may be no net societal health gains for a life-extending treatment for brain damage.
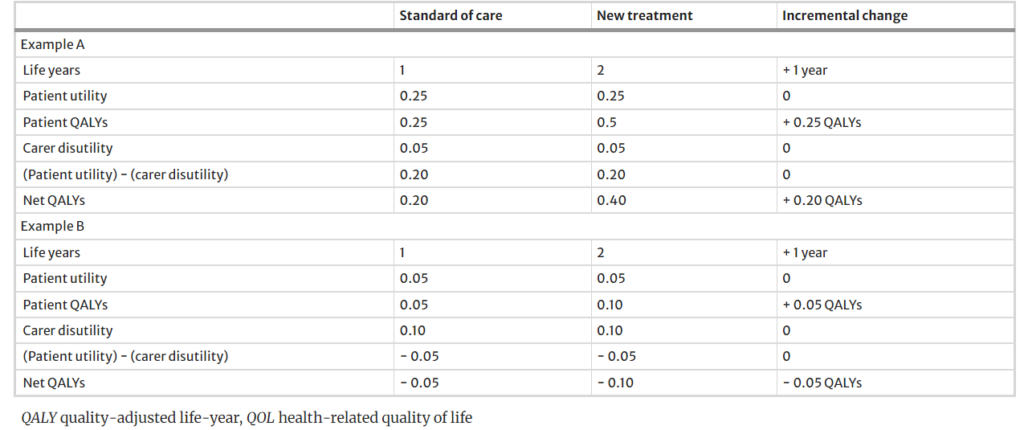
A numerical example from Mott et al. is below.
https://link.springer.com/article/10.1007/s40273-023-01316-0
The authors note that this is not just a theoretical problem:
In two recent National Institute for Health and Care Excellence (NICE) technology appraisals (TA588 and TA755), the inclusion of carer QOL in the economic models resulted in fewer QALYs being accrued with the new treatment, contributing to the treatment being deemed not cost effective. The implication was that life-extending treatments may not represent an efficient use of resources, at least in part due to the negative QALY impact that they would have on informal carers.
While caregiving for a disabled individual may decrease momentary utility–since it is both physically and emotionally hard work–carers quality of life could improve if we consider altruism effects (positive value of extending life of a loved one) or the bereavement effects (negative impact of the death) in the calculation. As an economist, I certainly rely on numerical analyses to evaluate treatment value; however, the carer QALY trap highlights that contextual considerations and qualitative information are needed to supplement the qualitative analysis whenever you are conducting health technology assessment.







