Medicaid and Racial Health Equity – Kaiser Family Foundation
The COVID-19 pandemic has highlighted and exacerbated longstanding racial and ethnic disparities in health and health care. Prior to the pandemic, people of color fared worse than White people across many measures of health and health care, reflecting inequities within the health care system as well as across broader social and economic factors that drive health (often referred to as social determinants of health) that are rooted in racism and discrimination. As a major source of health coverage for people of color, Medicaid programs can help to address health disparities. And, during the pandemic Medicaid enrollment has increased, reflecting both changes in the economy as well as “maintenance of eligibility” requirements included in the Families First Coronavirus Response Act (FFCRA). In the past year, the federal government and many states have identified advancing health equity as a key priority for the Medicaid program. This issue brief provides greater insight into the role Medicaid can play in advancing racial health equity by answering three key questions:
How does health coverage vary by race and ethnicity?
How can Medicaid help to reduce racial health disparities?
What are key issues to watch looking ahead?
How does health coverage vary by race and ethnicity?
Reflecting large coverage gains under the Affordable Care Act coverage expansions, including the Medicaid expansion to low-income adults, Medicaid plays a disproportionately large role in covering people of color (Figure 1). Most people of color have a full-time worker in the family, but they are more likely than White people to be employed in low-wage jobs that are less likely to offer health insurance. Moreover, people of color may face increased challenges affording private coverage because they are more likely to be low-income. While private insurance is the largest source of health coverage for people across racial and ethnic groups, people of color are less likely to be privately-insured than White people. Medicaid and the Children’s Health Insurance Program (CHIP) help to fill these gaps in private coverage for people of color and are the primary sources of coverage for some children of color. As of 2020, Medicaid covers about three in ten Black, American Indian and Alaska Native (AIAN), and Native Hawaiian or Other Pacific Islander (NHOPI) nonelderly adults and more than two in ten of Hispanic nonelderly adults, compared to 17% of their White counterparts. Reflecting more expansive eligibility levels for children compared to adults, Medicaid and CHIP play an even larger role for children of color, covering over half of Hispanic, Black, and AIAN children and nearly half of NHOPI children, compared to 27% of White children.
As a major source of coverage for people of color, the Medicaid program helps to ensure access to care and provide financial protection from health care costs. Research shows that having health insurance makes a key difference in whether, when, and where people get medical care. Uninsured people are far more likely than those with insurance to postpone health care or forgo it altogether. Being uninsured can also have financial consequences, with many unable to pay their medical bills, resulting in medical debt. However, research also shows that beyond health care coverage, broader social and economic factors outside the health care system play a major role in shaping health.
How can Medicaid help to reduce racial health disparities?
As noted, the federal government and states have identified addressing racial health equity as a key priority, including through Medicaid. While private insurance is the largest source of coverage for people of color, Medicaid can help to address health disparities through a range of tools available to policymakers.
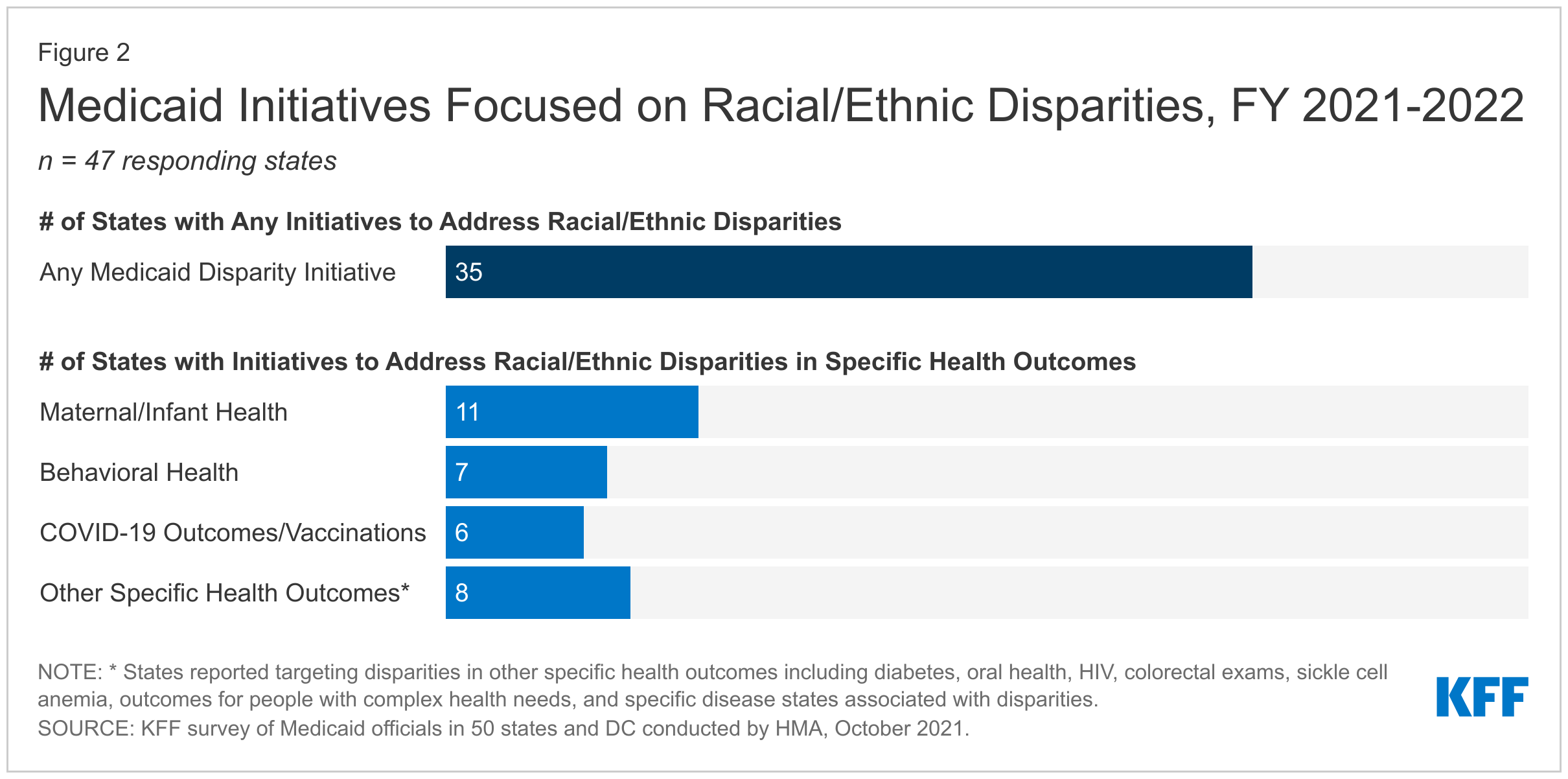
After taking office, President Biden issued a series of executive orders and actions focused on advancing equity and strengthening Medicaid. In November 2021, the Centers for Medicare and Medicaid Services (CMS) published its strategic vision for Medicaid and CHIP that identifies equity as one of three focus areas, connected to the two other areas of coverage and innovation. The Biden Administration has also emphasized equity as a key goal of Section 1115 waivers, which provide states an avenue to test new approaches in Medicaid not otherwise allowed under federal rules. In addition, the CMS Innovation Center has recently said it aims to embed health equity in every aspect of its payment and service delivery models. Many states also are focused on addressing racial disparities in Medicaid. On KFF’s 21st annual Medicaid budget survey fielded in the summer of 2021, three-quarters of responding states (35 of 47) reported Medicaid initiatives to address racial health disparities, sometimes focused on specific health outcomes (Figure 2). Many states are prioritizing health equity broadly across their Medicaid program, with initiatives to address disparities reported across numerous programmatic areas. Also, several states reported statewide equity initiatives that include but also extend beyond Medicaid, such as statewide equity taskforces or multi-agency initiatives across health and other sectors.
Actions taken across different areas of the Medicaid program may help advance this focus on mitigating racial disparities, including efforts to increase access to health coverage; pursuit of new approaches through Section 1115 waivers; and implementation of changes to managed care arrangements, provider payments, and benefits.
Access to Health Coverage
One significant action that would help close coverage disparities for people of color is adoption of the ACA Medicaid expansion in the 12 non-expansion states. As of 2014, the ACA expanded Medicaid to adults with incomes through 138% of the federal poverty level ($18,754 annually for an individual in 2022). Research suggests that Medicaid expansion is linked to increased access to care, improvements in some health outcomes, and has contributed to reductions in racial disparities in health coverage. However, as of February 2022, 12 states have not yet adopted the Medicaid expansion. In these non-expansion states, 2.2 million people fall in a coverage gap, with incomes too high to qualify for Medicaid but too low to qualify for Marketplace subsidies. Nationally, nearly six in ten people in the coverage gap are people of color (Figure 3). In particular, uninsured Black adults are more likely than their White counterparts to fall into the gap (15% vs. 8%) because most states that have not expanded Medicaid are in the South where a larger share of the Black population resides. The American Rescue Plan Act (ARPA) enacted in March 2021 includes a temporary fiscal incentive to encourage states to take up the expansion. While no state has newly adopted expansion since ARPA was enacted, this incentive reignited discussion around expansion in a few state legislatures. Also, in some states, advocates are pursuing expansion via ballot initiatives. The Build Back Better Act, which has passed the House but faces an uncertain future in the Senate, would temporarily close the Medicaid coverage gap by making low-income people in states that have not expanded Medicaid eligible for subsidized coverage in the ACA marketplace.
Other expansions of Medicaid eligibility could also address racial disparities in coverage and access to care. Medicaid covers more than 40% of births nationally, including more than two-thirds among Black and American Indian and Alaska Native (AIAN) individuals, who have higher rates of pregnancy-related mortality and morbidity as compared to White individuals. Because pregnancy-related Medicaid eligibility is limited to 60 days postpartum and Medicaid eligibility is much more restrictive for parents compared to pregnant people, especially in states that have not implemented the ACA Medicaid expansion, people can often lose coverage at the end of the postpartum period. ARPA includes a new option for states to extend pregnancy-related Medicaid coverage from 60 days postpartum to 12 months, beginning in April 2022, which could decrease the share of people becoming uninsured at the end of the 60-day postpartum period. At least 26 states plan to take up the ARPA option or otherwise extend postpartum coverage via a Section 1115 waiver. States have also reported that other Medicaid eligibility expansions for high-need populations may mitigate racial and ethnic disparities, such as pending Section 1115 waiver requests in seven states (AZ, CA, KY, MA, MT, UT, and VT) to allow for pre-release coverage of services for Medicaid-eligible individuals who are incarcerated—a population disproportionately composed of people of color.
Making it easier for eligible people to enroll in and maintain Medicaid coverage may also help close coverage gaps for people of color. The ACA simplified and streamlined Medicaid and CHIP enrollment and renewal requirements and procedures. Consistent with these requirements, many states have implemented changes to make it easier for eligible individuals to enroll in and maintain their coverage. In December 2021, the Biden Administration issued an Executive Order focused on reducing administrative burdens and making it easier for people to access services across federal agencies, including streamlining enrollment and renewal processes for health coverage. It also launched outreach and education campaigns and restored funding for Navigators to help eligible people enroll in health coverage. The Administration has also reversed some policies that may have contributed to coverage barriers for eligible individuals. For example, it reversed changes to public charge policies made under the Trump Administration, which had made immigrant families more reluctant to enroll in health coverage and other programs even if they were eligible. In addition, CMS has withdrawn Medicaid work requirement waivers in all states that had approvals, a decision based in part on data indicating racial disparities in job and income loss and negative health outcomes during the pandemic. More recently, CMS took steps to withdraw or phase out waivers with Medicaid premium requirements above statutory limits, citing research finding that these premium policies can exacerbate disparities in coverage and access to care. Together, these actions may help to close remaining coverage gaps for people of color by making it easier for eligible people to enroll and maintain coverage. In 2020, nearly two-thirds of the seven million uninsured people were eligible for Medicaid but not enrolled were people of color (Figure 4).
Section 1115 Waivers
The Biden Administration and states may pursue equity-related initiatives through Section 115 waivers. As noted, Section 1115 demonstration waivers provide an avenue to test new approaches in Medicaid. Waivers generally reflect state priorities as well as shifting priorities from one presidential administration to another. The Biden Administration has emphasized equity as a key goal of Section 1115 waivers. For example, the administration has highlighted a commitment to improving maternal health disparities with its approvals of waivers extending Medicaid postpartum coverage prior to the ARPA option becoming available. The administration also noted that its recent renewals of California’s CalAIM demonstration and Maryland’s HealthChoice demonstration would advance health equity, in part, by addressing maternal health and health-related social needs. The California approval also included new equity protocols for the state’s Global Payment Program, which aims to support lower cost, efficient, and equitable health care to the state’s uninsured population. The Biden Administration may also act on pending waiver requests that identify health equity as a foundational goal underlying all or most provisions (Figure 5). In particular, states have highlighted that pending requests to expand coverage for high-need populations and increase support for social determinants of health will promote health equity. In addition, some states have requested provisions specifically aimed at measuring or incentivizing equity. For example, Massachusetts and Vermont are requesting expenditure authority related to improved data collection and reporting for health disparities.
Managed Care, Provider Payments, and Benefits
States can leverage managed care contracts to help address racial disparities and social determinants of health. Over two-thirds of Medicaid beneficiaries are enrolled in comprehensive, risk-based managed care organizations (MCOs) nationally. Analysis suggests that, among Medicaid managed care enrollees, people of color experience worse care experiences than White enrollees. However, states can establish requirements for MCOs aimed at reducing disparities. For example, states develop access and quality standards within federal guidelines that MCOs are required to meet. In particular, since 2016 states that contract with managed care plans have been required to develop and post publicly quality strategies that include plans to reduce health care disparities. States must also require MCOs to implement performance improvement projects (PIPs) to examine access to and quality of care, though specific PIP focus areas vary across states and plans. On KFF’s 2021 budget survey, several states reported PIPs focused on addressing racial health disparities. States also are incorporating requirements into MCO contracts with the goal of advancing health equity, such as requiring MCOs to achieve the NCQA Distinction in Multicultural Health Care. Additionally, the vast majority of states that contract with MCOs reported leveraging these contracts to address social determinants of health, which are important for improving health and reducing health disparities (Figure 6). For example, more than half of responding states reported requiring MCOs to screen enrollees for social and behavioral health needs, to provide referrals to social services, and to partner with community-based organizations. In addition, states can use specific payment options for MCOs to help address social needs. Although federal Medicaid rules prohibit expenditures for most non-medical services, states can allow MCOs to pay for limited non-medical services through “in-lieu-of services” (ILOS) authority and/or “value-added” services. For example, CMS recently authorized a set of managed care ILOS called Community Supports in California to address social drivers of health, a step the state identifies as “key to advancing health equity.” These include services such as housing supports, personal care, medically supportive food assistance, and home modifications.
States can also adopt health plan and provider payment options to incentivize reductions in racial health disparities. States incorporate quality metrics into ongoing monitoring of their Medicaid programs across delivery systems (fee-for-service and managed care), including linking financial incentives like performance bonuses or penalties, capitation withholds, or value-based state-directed payments to quality measures. As of July 1, 2021, 12 states reported linking financial incentives to health disparities metrics, an increase from just two states two years ago (Figure 7). Most of these states indicated that the disparities-related financial incentives were in their managed care delivery systems. State activity tying provider payment increases to health disparities may continue to increase. For example, Massachusetts is requesting a new Section 1115 waiver amendment to provide incentive payments to provider networks and hospitals that collect accurate social risk factor data, identify and monitor inequities through stratified data reporting, and achieve measurable reductions in health disparities.
Expansions of Medicaid benefits and telehealth may increase access to care for all enrollees, including the disproportionate share of people of color covered by Medicaid. KFF’s 2021 budget survey found many states reporting Medicaid benefit expansions, including benefits that may help reduce disparities. For example, states are expanding pregnancy and postpartum services, housing and housing-related supports, and community health worker services. States are also adding benefits to address behavioral health conditions (including mental illnesses and substance use disorder (SUD)), which have disproportionately affected people of color both during and prior to the COVID-19 pandemic. For example, most states are expanding services that aim to connect Medicaid enrollees experiencing mental health crises to appropriate community-based care, often as an alternative to responses by law enforcement. In addition to benefit expansions, many states have expanded allowances of telehealth in Medicaid to promote access to care during the COVID-19 pandemic. Recent research finds that telehealth use rates during the pandemic have been highest among Medicaid enrollees and individuals who identify as Black, Hispanic, or multiracial. Coverage of audio-only telehealth may play a particularly important role in addressing racial disparities. AIAN, Black, NHOPI, and Hispanic Medicaid enrollees are all significantly more likely than White enrollees to have limited internet or computer access, and other data show that during the pandemic video telehealth rates have been lowest among Black, Asian, and Hispanic individuals.
What are key issues to watch looking ahead?
It will be important to help prevent the end of the COVID-19 public health emergency (PHE) from resulting in coverage losses that widen disparities for people of color. Provisions in the Families First Coronavirus Response Act (FFCRA) require states to maintain continuous Medicaid enrollment for enrollees until the end of the month when the COVID-19 PHE ends. When the continuous enrollment requirements end and states resume redeterminations and disenrollments, some people may lose Medicaid coverage or experience a gap in coverage due to barriers completing these processes, even if they remain eligible for coverage. Some individuals may be at increased risk of losing coverage due to administrative barriers, including people with Limited English Proficiency, people who move frequently, or people with fluctuating incomes. As such, to ensure that the PHE does not result in coverage losses that widen racial disparities, it will be important for states to take steps to eliminate and reduce potential administrative barriers and working closely with community partners to conduct outreach and enrollment assistance.
Congress could pass Medicaid-related provisions proposed in the Build Back Better Act (BBBA) that may further advance efforts to address racial health disparities. The BBBA that passed the House in November 2021 includes a provision that would temporarily allow people in the coverage gap to purchase subsidized coverage (with no premiums and minimal cost sharing) in the ACA Marketplace. In addition, the BBBA would require 12 months of continuous coverage for postpartum individuals and children. The BBBA would also partially lift the inmate exclusion (current policy that prohibits Medicaid from covering services provided to Medicaid eligible people while incarcerated, except for inpatient services) by allowing federal Medicaid money to be used to pay for Medicaid-covered services 30 days prior to release for people who are incarcerated—a population disproportionately composed of people of color. Finally, the BBBA proposes provisions that would expand access to behavioral health care and potentially address disparities in this area. The fate of the BBBA’s policy changes remains uncertain in the Senate.
Absent federal legislation, the Biden Administration may continue to advance its equity priorities through administrative actions. As noted above, CMS could approve pending Section 1115 waiver requests that directly and indirectly seek to reduce racial health disparities. The administration has signaled it is working to develop a clear set of Section 1115 policy principles; such guidance could encourage states to submit additional waiver requests focused on health equity. Beyond waivers, CMS recently announced a Request for Information to inform development of a comprehensive Medicaid and CHIP access strategy to advance health equity.
Improving Medicaid data collection and reporting will be key for addressing racial health disparities. Comprehensive disaggregated data are essential for identifying disparities, directing efforts and resources to address disparities as they are identified, measuring progress toward achieving greater equity, and establishing accountability for achieving progress. Without adequate data, inequities remain unseen and unaddressed. However, to date, there have been major gaps and limitations in Medicaid and CHIP data available to identify and address racial disparities. For example, analysis of administrative data finds high rates of missing or unknown racial and ethnic data and conflicts with key benchmark data. Further, with over two-thirds of Medicaid beneficiaries enrolled in MCOs nationally, MCO performance is key to addressing racial health equity for enrollees; however, detailed MCO performance information at the plan-level is not frequently made publicly available by state Medicaid agencies, especially disaggregated by race and ethnicity. Looking ahead, improvements to data collection and transparency will be central to efforts to address disparities.
While Medicaid can play a key role in helping to address racial disparities in health and health care, broader efforts within and beyond the health care system will also be important. Disparities in health and health care remain a persistent issue beyond the Medicaid program, reflecting historic and ongoing racism. Many of these underlying disparities placed people of color at increased risk for negative health and economic impacts from the COVID-19 pandemic. Moreover, the pandemic has exacerbated many of these disparities and may continue to contribute to widening disparities in the future. As a major source of health coverage for people of color, Medicaid can play a significant role in helping to address racial health disparities. However, broader efforts to address structural racism and inequities across the health care system and social and economic factors that drive health will also be necessary for advancing health equity.







